Fluid Management


必须有适当的动脉压和心输出量(CO)才能达到适当的灌注
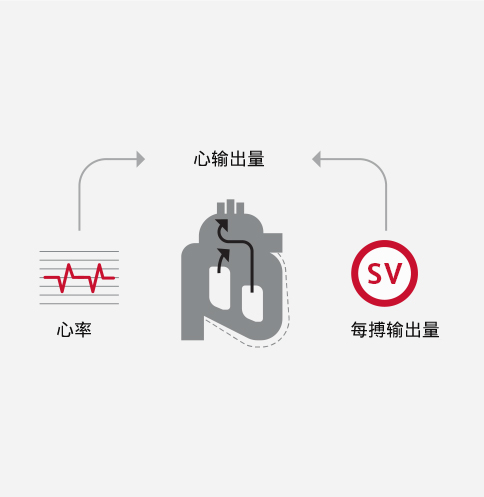
心输出量(CO)=每搏输出量×心率
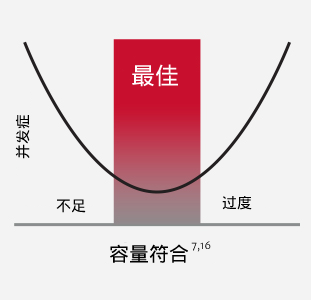
关键在于使患者保持在最佳容量范围内。使用基于流量的动态参数来指导液体管理,有助于使患者保持在最佳容量范围内。1
容量不足与下列各项相关:
- 胃肠道功能障碍(术后肠梗阻、术后恶心呕吐(PONV)、上消化道出血、吻合口瘘)2
- 感染性并发症(组织灌注不足)2,3
- 急性肾功能不全或肾衰竭4
容量过度与下列各项相关:
- 肺水肿5
- 胃肠道功能障碍(腹腔室隔综合征、肠梗阻、吻合口瘘)17,18,19
- 凝血功能障碍5
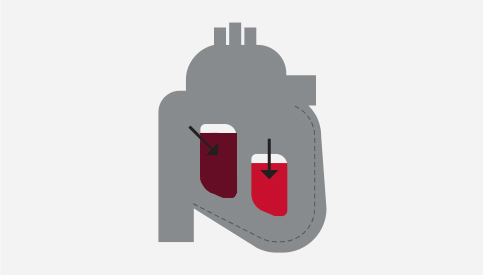
前负荷:舒张末期心肌纤维的张力,是心室容积的结果
每搏输出量(SV):每次心搏时从左心室泵出的血量
管理灌注时,可以使用患者自己的Frank-Starling曲线(每搏量输出量(SV)vs.前负荷的曲线)来优化每搏输出量。
位于Frank-Starling曲线肩部时,每搏输出量是最佳的(参见下图)。
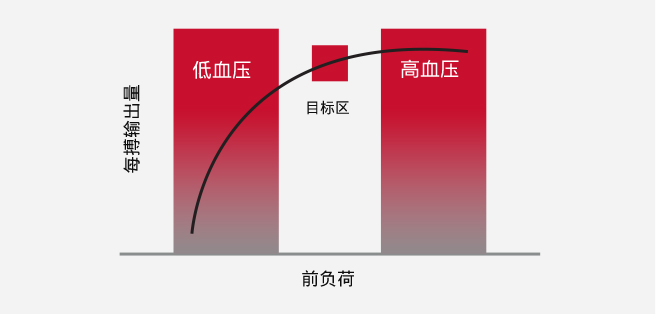
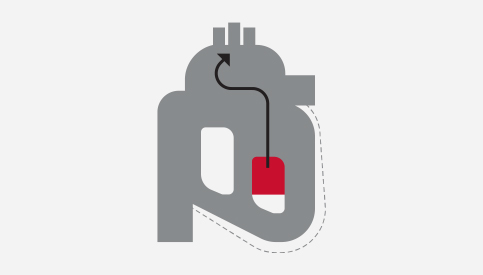
通过采用下列方式,测量对前负荷变化的反应(∆SV),可以确定患者在其Frank-Starling曲线上的位置:
液体推注挑战
被动抬腿实验(PLR)
就确定液体反应性而言,基于流量的动态参数提供的信息多于常规参数,并且可能有助于避免输液过量或不足。7
临床研究表明,基于常规参数的常规容量管理方法存在误导性且不敏感。6
每搏输出量(SV)和每搏量变异度(SVV)等高级血流动力学参数是优化液体管理的关键。6
已证明SVV是管理灌注时对前负荷反应具有高度敏感性和特异性的指标。SVV是一项动态参数,已证明可作为机械通气引起的负载条件下液体反应性的准确预测指标。6,8,20
- Thacker, et al. Perioperative Fluid Utilization Variability and Association With Outcomes: Considerations for Enhanced Recovery Efforts in Sample US Surgical Population. Ann Surg 2015
- Peng, K., et al., Goal-directed fluid therapy based on stroke volume variations improves fluid management and gastrointestinal perfusion in patients undergoing major orthopedic surgery. Med Princ Pract, 2014
- Dalfino et al. Haemodynamic goal-directed therapy and postoperative infections: earlier is better. A systematic review and meta-analysis. Crit Care 2011
- Giglio, MT et al. Goal-directed haemodynamic therapy and gastrointestinal complications in major surgery: a meta-analysis of randomized controlled trials. British Journal of Anesthesia 2009
- Shin, C. et al. Effects of Intraoperative Fluid Management on Postoperative Outcomes: A Hospital Registry Study. Annals of Surgery 2017
- Sun, Y. et al. Effect of perioperative goal-directed hemodynamic therapy on postoperative recovery following major abdominal surgery-a systematic review and meta-analysis of randomized controlled trials. Critical Care 2017
- Goepfert, M.S., et al., Individually optimized hemodynamic therapy reduces complications and length of stay in the intensive care unit: a prospective, randomized controlled trial. Anesthesiology, 2013
如需了解关于使用高级参数管理液体的更多信息,请联系我们。

术后并发症会对人们的生活造成影响。9


约16%的手术会出现重大并发症。9
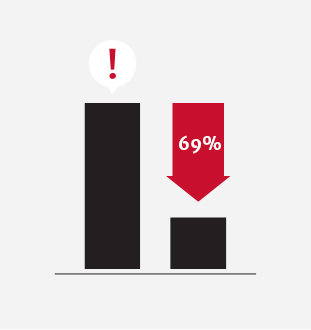
在不考虑患者术前风险的情况下,即使在30天内发生单一术后并发症,患者的中位生存率也会降低69%。10
已证明通过PGDT优化血流动力学可以减少急性肾损伤(AKI)和手术部位感染(SSI)等并发症,并减少中高风险手术患者的住院时长和相关费用。11,12
通过PGDT优化血流动力学可以:


术后并发症平均减少32%13
缩短平均住院时长:1天以上13,14
治疗一种术后并发症的额外费用约为:$18,0000 - $20,00015
PGDT是使用基于流量的动态血流动力学参数的治疗方案,目的是做出适当的容量管理决策。可以在单一手术操作中进行PGDT,也可以将其作为更大项目(例如:增强术后恢复途径)的一部分。
50多项研究证明了PGDT的使用
50多项随机对照试验和14多项荟萃分析已证明血流动力学优化的临床获益大于标准容量管理。
研究
- Michard, et al. Perioperative goal-directed therapy with uncalibrated pulse contour methods: impact on fluid management and postoperative outcome. British Journal of Anesthesia 2017
- Pearse, R. et al. Effect of a Perioperative, Cardiac Output–Guided Hemodynamic Therapy Algorithm on Outcomes Following Major Gastrointestinal Surgery A Randomized Clinical Trial and Systematic Review. JAMA 2014
- Grocott, MP et al. Perioperative increase in global blood flow to explicit defined goals and outcomes after surgery: a Cochrane Systematic Review. British Journal of Anesthesia 2013
- Thiele et al. American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on perioperative fluid management within an enhanced recovery pathway for colorectal surgery. Periop Med 2016
- Ramsingh , et al. Outcome impact of goal directed fluid therapy during high risk abdominal surgery in low to moderate risk patients: a randomized controlled trial. J Clin Monit Comput 2011
- Cecconi, et al. Goal directed haemodynamic therapy during elective total hip arthroplasty under regional anaesthesia. Crit Care 2011
证明围手术期目标导向治疗获益的随机对照试验
52项阳性随机对照试验中入组3000多名患者。
| PAC, n = 8 (1175 名患者) |
多普勒, n = 12 (1145 名患者) |
脉搏曲线, n=29 (2621 名患者) |
A line, n = 1 (33 名患者) |
CVC, n = 2 (214 名患者) |
| 标题、作者和年份 | n | 优化的参数 | 外科手术 | 工具 | 主要获益 |
|---|---|---|---|---|---|
| Prospective trial of supranormal values of survivors as therapeutic goals in high-risk patients. Shoemaker 1988 | 310 | DO2 | 普外 | PAC-1 | 发病率 死亡率(21 vs 34%) 节省成本 |
| Preoperative optimization of cardiovascular hemodynamics improves outcomes in peripheral vascular surgery. Berlauk 1991 | 89 | CI, PCWP, SVR | 血管 | PAC-2 | 发病率 |
| Prospective trial of supranormal values as goals of resuscitation in severe trauma. Fleming 1992 | 67 | DO2 | 创伤 | PAC-3 | 发病率 |
| A randomized clinical trial of the effect of deliberate perioperative increase of oxygen delivery on mortality in high-risk patients. Boyd 1993 | 107 | DO2 | 普外 | PAC-4 | 发病率 死亡率(6 vs 22%) |
| Perioperative plasma volume expansion reduces the incidence of gut mucosal hypoperfusion during cardiac surgery. Mythen 1995 | 60 | SV | 心脏 | 多普勒-1 | 发病率 医院住院时长 |
| Intraoperative intravascular volume optimisation and length of hospital stay after repair of proximal femoral fracture: randomised controlled trial. Sinclair 1997 | 40 | SV | 髋关节 | 多普勒-2 | 医院住院时长 |
| Response of patients with cirrhosis who have undergone partial hepatectomy to treatment aimed at achieving supranormal oxygen delivery and consumption. Ueno 1998 | 34 | DO2 | 肝切除 | PAC-5 | 发病率 |
| Reducing the risk of major elective surgery: randomised controlled trial of preoperative optimization of oxygen delivery. Wilson 1999 | 138 | DO2 | 普外和血管 | PAC-6 | 发病率 医院住院时长 节省成本 |
| A prospective, randomized study of goal-oriented hemodynamic therapy in cardiac surgical patients. Polonen 2000 | 393 | SvO2 | 心脏 | PAC-7 | 发病率 医院住院时长 |
| Effects of maximizing oxygen delivery on morbidity and mortality in high-risk surgical patients. Lobo 2000 | 37 | DO2 | General | PAC-8 | 发病率 死亡率(16 vs 50%) |
| Randomized controlled trial to investigate influence of the fluid challenge on duration of hospital stay and perioperative morbidity in patients with hip fractures. Venn 2002 | 59 | SV | 髋关节 | 多普勒-3 | 发病率 |
| Goal-directed Intraoperative fluid administration reduces length of hospital stay after major surgery. Gan 2002 | 100 | SV | 普外 | 多普勒-4 | 发病率 医院住院时长 |
| Randomised controlled trial investigating the influence of intravenous fluid titration using oesophageal Doppler monitoring during bowel surgery. Conway 2002 | 57 | SV | 肠道 | 多普勒-5 | 发病率 |
| Randomised controlled trial assessing the impact of a nurse delivered, flow monitored protocol for optimisation of circulatory status after cardiac surgery. McKendry 2004 | 174 | SV | 心脏 | 多普勒-6 | 医院住院时长 |
| Intraoperative oesophageal Doppler guided fluid management shortens postoperative hospital stay after major bowel surgery. Wakeling 2005 | 128 | SV | 肠道 | 多普勒-7 | 发病率 医院住院时长 |
| Early goal-directed therapy after major surgery reduces complications and duration of hospital stay. A randomised, controlled trial. Pearse 2005 | 122 | DO2 | 普外 | LidCO-1 | 发病率 医院住院时长 |
| Randomized clinical trial assessing the effect of Doppler- optimized fluid management on outcome after elective colorectal resection. Noblett 2006 | 108 | SV | 肠道 | 多普勒-8 | 发病率 医院住院时长 |
| Esophageal Doppler-guided fluid management decreases blood lactate levels in multiple-trauma patients: a randomized controlled trial. Chytra 2007 | 162 | SV | 创伤 | 多普勒-9 | 发病率 医院住院时长 |
| Goal-directed fluid management based on pulse pressure variation monitoring during high-risk surgery: a pilot randomized controlled trial. Lopes 2007 | 33 | PPV | 普外 | A line-1 | 发病率 医院住院时长 |
| Goal-directed intraoperative therapy reduces morbidity and length of hospital stay in high-risk surgical patients. Donati 2007 | 135 | ERO2 | 普外和血管 | CVC-1 | 发病率 医院住院时长 |
| Goal-directed intraoperative therapy based on Autocalibrated arterial pressure waveform analysis reduces hospital stay in high-risk surgical patients: a randomized, controlled trial. Mayer 2009 | 60 | SVV, SVI, CI | 腹部 | FloTrac传感器-1 | 发病率 医院住院时长 |
| Intraoperative fluid optimization using stroke volume variation in high risk surgical patients: results of prospective randomized study. Benes 2010 | 120 | SVV, CI | 腹部和血管 | FloTrac传感器-2 | 发病率 |
| Haemodynamic optimisation improves tissue microvascular flow and oxygenation after major surgery: a randomised controlled trial. Jhanji 2010 | 135 | SV, DO2 | 腹部 | LidCO-2 | 发病率 |
| Goal-directed haemodynamic therapy during elective total hip arthroplasty under regional anaesthesia. Cecconi 2011 | 40 | DO2 | 髋关节 | FloTrac传感器-3 | 发病率 |
| A double-blind randomized controlled clinical trial to assess the effect of doppler optimized intraoperative fluid management on outcome following radical cystectomy. Pillai 2011 | 66 | SV | 膀胱切除术 | 多普勒-10 | 发病率 |
| Haemodynamic optimisation in lower limb arterial surgery: room for improvement? Bisgaard 2012 | 40 | SV, DO2 | 血管 | LidCO-3 | 发病率 |
| Outcome impact of goal directed fluid therapy during high risk abdominal surgery in low to moderate risk patients: a randomized controlled trial. Ramsingh 2012 | 38 | SVV | 腹部 | FloTrac传感器-4 | 发病率 医院住院时长 |
| Goal-directed intraoperative fluid therapy guided by stroke volume and its variation in high-risk surgical patients: a prospective randomized multicentre study. Scheeren 2012 | 40 | SVV, SV | 腹部 | FloTrac传感器-5 | 发病率 |
| Intraoperative fluid management in open gastrointestinal surgery: goal-directed versus restrictive. Zhang 2013 | 80 | SVV, CI | 胸部 | FloTrac传感器-6 | 发病率 |
| Individually optimized hemodynamic therapy reduces complications and length of stay in the Intensive Care Unit. Goepfert 2013 | 100 | SVV, GEDI, CI, EVLW | 心脏 | PiCCO-1 | 发病率 |
| Perioperative goal-directed hemodynamic therapy based on radial arterial pulse pressure variation and continuous cardiac index trending reduces postoperative complications after major abdominal surgery: a multi-center, prospective, randomized study. Salzwedel 2013 | 160 | PPV, CI | 腹部 | ProAQT-1 | 发病率 医院住院时长 |
| Goal-directed fluid therapy in gastrointestinal surgery in older coronary heart disease patients: randomized trial. Zheng 2013 | 60 | SVV, SVI, CI | 腹部 | FloTrac传感器-7 | 发病率 医院住院时长 |
| Zakhaleva, J., et al., The impact of intravenous fluid administration on complication rates in bowel surgery within an enhanced recovery protocol: a randomized controlled trial. Colorectal Dis, 2013. 15(7): p. 892-9 | 91 | SV | 腹部外科 | TED | 发病率 |
| Peng, K., et al., Goal-directed fluid therapy based on stroke volume variations improves fluid management and gastrointestinal perfusion in patients undergoing major orthopedic surgery. Med Princ Pract, 2014. 23(5): p. 413-20 | 80 | SVV | 骨外科 | PC FloTrac传感器 | 胃肠道恢复 |
| Zeng, K., et al., The influence of goal-directed fluid therapy on the prognosis of elderly patients with hypertension and gastric cancer surgery. Drug Des Devel Ther, 2014. 8: p. 2113-9 | 60 | SVV | 胃切除术 | PC FloTrac传感器 | 发病率,医院住院时长 |
| Colantonio, L., et al., A randomized trial of goal directed vs. standard fluid therapy in cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. J Gastrointest Surg, 2015. 19(4): p. 722-9 | 80 | CI, SVI | 细胞减数外科 | PC FloTrac传感器 | 发病率,医院住院时长 |
| Funk, D.J., et al., A randomized controlled trial on the effects of goal-directed therapy on the inflammatory response open abdominal aortic aneurysm repair. Crit Care, 2015. 19: p. 247 | 40 | SVV, CI | 血管外科 | PC FloTrac传感器 | 发病率 |
| Mikor, A., et al., Continuous central venous oxygen saturation assisted intraoperative hemodynamic management during major abdominal surgery: a randomized, controlled trial. BMC Anesthesiol, 2015. 15: p. 82 | 79 | ScvO2 | 腹部外科 | CVC Cevox | 死亡率和氧供 |
| Han, G., et al., Application of LiDCO-Rapid in peri-operative fluid therapy for aged patients undergoing total hip replacement. International Journal of Clinical and Experimental Medicine, 2016. 9(2): p. 4473-4478 | 40 | SVV | 骨外科 | PC LiDCO rapid | 发病率 |
| Hand, W.R., et al., Intraoperative goal-directed hemodynamic management in free tissue transfer for head and neck cancer. Head Neck, 2016. 38 Suppl 1: p. E1974-80 | 94 | SVV, CI, SVR | 游离组织外科 | PC FloTrac传感器 | ICU住院时长 |
| Kapoor, P.M., et al., Perioperative utility of goal-directed therapy in high-risk cardiac patients undergoing coronary artery bypass grafting: “A clinical outcome and biomarker- based study”. Ann Card Anaesth, 2016. 19(4): p. 638-682 | 130 | SVV, CI, SVI, SVRI, DO2 | 心脏外科 | PC FloTrac传感器,中心静脉血氧饱和度导管(CVC) | ICU住院时长,医院住院时长 |
| Kumar, L., S. Rajan, and R. Baalachandran, Outcomes associated with stroke volume variation versus central venous pressure guided fluid replacements during major abdominal surgery. J Anaesthesiol Clin Pharmacol, 2016. 32(2): p. 182-6 | 60 | SVV | 腹部外科 | PC FloTrac传感器 | ICU住院时长 |
| Osawa, E.A., et al., Effect of Perioperative Goal-Directed Hemodynamic Resuscitation Therapy on Outcomes Following Cardiac Surgery: A Randomized Clinical Trial and Systematic Review. Crit Care Med, 2016. 44(4): p. 724-33 | 126 | CI, SVI | 心脏外科 | PC LidCO Rapid | 发病率,ICU住院时长,医院住院时长 |
| Yuanbo, Z., et al., ICU management based on PiCCO parameters reduces duration of mechanical ventilation and ICU length of stay in patients with severe thoracic trauma and acute respiratory distress syndrome. Annals of Intensive Care, 2016. 6(1): p. 113 | 264 | ITBVI, EVLWI, CI | ARDS ICU治疗 | PC PiCCO | MV天数,ICU住院时长,节省成本 |
| Elgendy, M.A., I.M. Esmat, and D.Y. Kassim, Outcome of intraoperative goal-directed therapy using Vigileo/FloTrac in high-risk patients scheduled for major abdominal surgeries: A prospective randomized trial. Egyptian Journal of Anaesthesia, 2017 | 86 | SVV, CI, MAP | 腹部大手术 | PC FloTrac传感器 | 发病率,ICU住院时长 |
| Kapoor, P.M., et al., Goal-directed therapy improves the outcome of high-risk cardiac patients undergoing off-pump coronary artery bypass. Ann Card Anaesth, 2017. 20(1): p. 83-89 | 163 | SVV, CI, ScvO2 | 心脏外科 | VolumeView套件,PC FloTrac传感器 | ICU住院时长,医院住院时长 |
| Kaufmann, K.B., et al., Oesophageal Doppler guided goal-directed haemodynamic therapy in thoracic surgery - a single centre randomized parallel-arm trial. Br J Anaesth, 2017. 118(6): p. 852-861 | 100 | SV, CI MAP | 胸外科 | TED | 发病率,医院住院时长 |
| Liang, M., et al., Effect of goal-directed fluid therapy on the prognosis of elderly patients with hypertension receiving plasmakinetic energy transurethral resection of prostate. Int J Clin Exp Med, 2017. 10(1): p. 1290-1296 | 60 | SVV | 泌尿外科-前列腺切除术 | PC FloTrac传感器 | 发病率,医院住院时长 |
| Luo, J., et al., Goal-directed fluid restriction during brain surgery: a prospective randomized controlled trial. Ann Intensive Care, 2017. 7(1): p. 16 | 145 | SVV, CI | 神经外科 | PC FloTrac传感器 | ICU住院时长,节省成本,发病率 |
| Weinberg, L., et al., Restrictive intraoperative fluid optimisation algorithm improves outcomes in patients undergoing pancreaticoduodenectomy: A prospective multicentre randomized controlled trial. PLoS One, 2017. 12(9): p. e0183313 | 52 | SVV, CI | 腹部 | PC FloTrac传感器 | 发病率,医院住院时长 |
| Wu, C.Y., et al., Comparison of two stroke volume variation-based goal-directed fluid therapies for supratentorial brain tumour resection: a randomized controlled trial. Br J Anaesth, 2017. 119(5): p. 934-942 | 80 | SVV | 神经外科 | PC FloTrac传感器 | ICU住院时长,发病率 |
| Wu, J., et al., Goal-directed fluid management based on the auto-calibrated arterial pressure-derived stroke volume variation in patients undergoing supratentorial neoplasms surgery. INTERNATIONAL JOURNAL OF CLINICAL AND EXPERIMENTAL MEDICINE, 2017. 10(2): p. 3106-3114 | 66 | SVV, CI, MAP | 脑外科 | PC FloTrac传感器 | 发病率 乳酸 |
Edwards临床教育
促进临床进步的血流动力学教育
始终致力于通过教育来改善外科和重症监护患者的护理质量,无论您在学习过程中的哪个阶段,Edwards临床教育都能向您提供一系列的资源和工具,在您目前和未来面临临床挑战时,可以为您不断提供支持。
- Benes, J., Giglio M., Michard, F. (2014) The effects of goal-directed fluid therapy based on dynamic parameters on post-surgical outcome: a meta-analysis of randomized controlled trials. Critical Care, 18(5), 584
- Giglio, MT., Marucci, M., Testini, M., Brienza, N. (2009) Goal-directed haemodynamic therapy and gastrointestinal complications in major surgery: a meta-analysis of randomized controlled trials. British Journal of Anaesthesia, 103(5), 637-46
- Johnson, A., Ahrens, T. (2015) Stroke Volume Optimization: The New Hemodynamic Algorithm. Critical Care Nurse, 35(1), 11-27
- O’Leary, M. (2001) Preventing renal failure in the critically ill. BMJ, 322(7300), 1437-1439
- Holte, K. (2010) Pathophysiology and clinical implications of perioperative fluid management in elective surgery. Danish Medical Bulletin, 57(7), B4156
- Berkenstadt, H., et al. (2001) Stroke Volume Variation as a Predictor of Fluid Responsiveness in Patients Undergoing Brain Surgery. Anesthesia & Analgesia, 92, 984-9
- Cannesson, M. (2010) Arterial pressure variation and goal-directed fluid therapy. Journal of Cardiothoracic and Vascular Anesthesia, 24(3), 487-97
- Peng, K., Li, J., Cheng, H., Ji, FH. (2014) Goal-directed fluid therapy based on stroke volume variations improves fluid management and gastrointestinal perfusion in patients undergoing major orthopedic surgery. Medical Principles and Practice, 23(5), 413-20
- Ghaferi, A., Birkmeyer, J., Dimick, J. (2009) Variation in hospital mortality associated with inpatient surgery. New England Journal of Medicine, 361(14), 1368-75
- Khuri, S., Henderson, W., DePalma, R., Mosca, C., Healey, N., Kumbhani, D. (2005) Determinants of long-term survival after major surgery and the adverse effect of postoperative complications. Annals of Surgery, 242(3), 326-41
- Aya, H., Cecconi, M., Hamilton, M., Rhodes, A. (2013) Goal-directed therapy in cardiac surgery: a systematic review and meta-analysis. British Journal of Anaesthesia, 110(4), 510-7
- Brienza, N., Giglio, M., Marucci, M., Fiore, T. (2009) Does perioperative hemodynamic optimization protect renal function in surgical patients? A meta-analytic study. Critical Care Medicine, 37(6), 2079-90
- Grocott, M., Dushianthan, A., Hamilton, M., Mythen, M., Harrison, D., Rowan, K. (2012) Perioperative increase in global blood flow to explicit defined goals and outcomes following surgery. Cochrane Database of Systematic Reviews, 11, CD004082
- Corcoran, T., Rhodes, J., Clarke, S., Myles, P., Ho, K. (2012) Perioperative fluid management strategies in major surgery: a stratified meta-analysis. Anesthesia & Analgesia, 114(3), 640-51
- Boltz, M., Hollenbeak, C., Ortenzi, G., Dillon, P. (2012) Synergistic implications of multiple postoperative outcomes. American Journal of Medical Quality, 27(5), 383-90
- Bellamy, M. (2006) Wet, dry or something else? British Journal of Anaesthesia, 97(6), 755-7
- Ping W, et al. Effects of Stroke Volume Variability-Guided Intraoperative Fluid Restriction on Gastrointestinal Functional Recovery. Chinese Journal of Anesthesiology 31.1 (2011): 78-81.
- Thacker JKM, et al. Perioperative Fluid Utilization Variability and Association With Outcomes. Annals of Surgery 263.3 (2016): 502-510.
- Durairaj L and Schmidt GA. Fluid Therapy in Resuscitated Sepsis*. Less is More. Recent Advances in Chest Medicine. 133.1 (2008): 252-263.
- Li, Cheng, et al. Stroke Volume Variation for Prediction of Fluid Responsiveness in Patients Undergoing Gastrointestinal Surgery. International Journal of Medical Sciences. 2013; 10(2): 148-155.
Please update your browser

Please update to a current version of your preferred browser, this site will perform effectively on the following:




If you are on a computer, that is maintained by an admin and you cannot install a new browser, ask your admin about it. If you can't change your browser because of compatibility issues, think about installing a second browser for browsing and keep this old one for compatibility