

连续的ScvO2监测
患者越小,就越需要早知道。
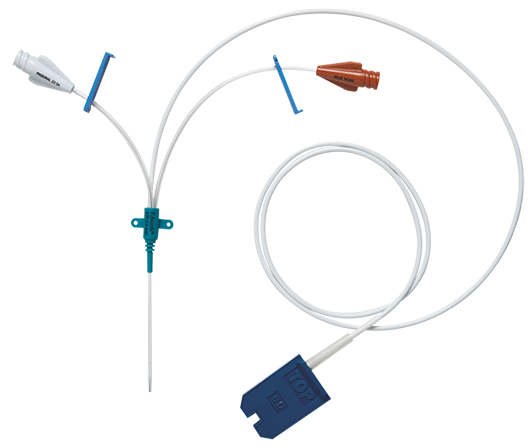
PediaSat 氧饱和度导管是第一个也是唯一的一个连续监测ScvO2,并进行积极的组织缺氧管理的儿科血氧饱和度导管。1-3
对中心静脉氧饱和度(ScvO2)进行连续、(化)实时监测,能够早期辨别氧供的关键变化,这是灵敏度较低的指标(如传统的生命体征或间歇式监测)不一定能辨别的。1‑9
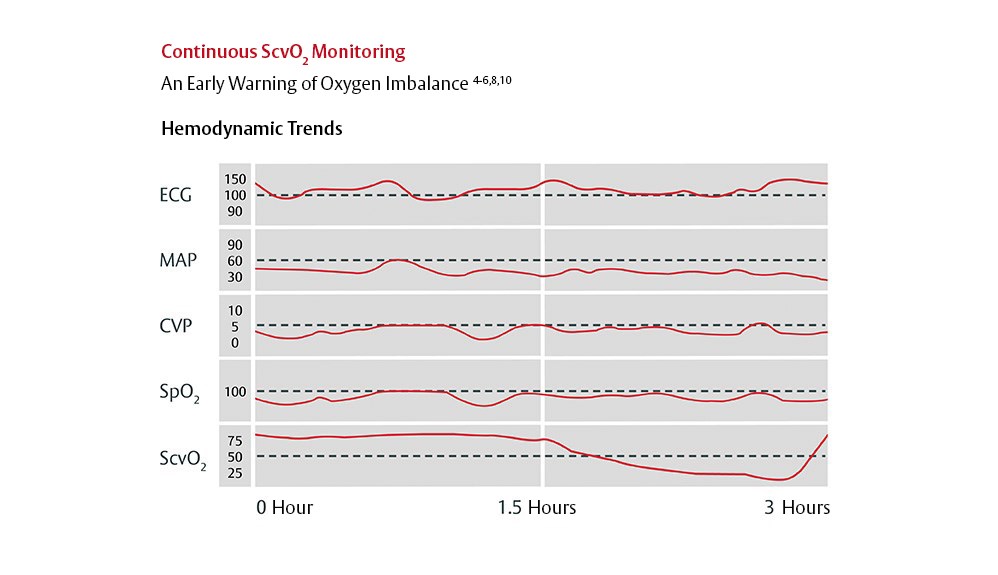
氧失衡早期预警为早期干预创造条件。
持续监测ScvO2作为早期指征,可以尽−早−甄别、预防复杂儿科患者的组织缺氧问题。4-6、8、10
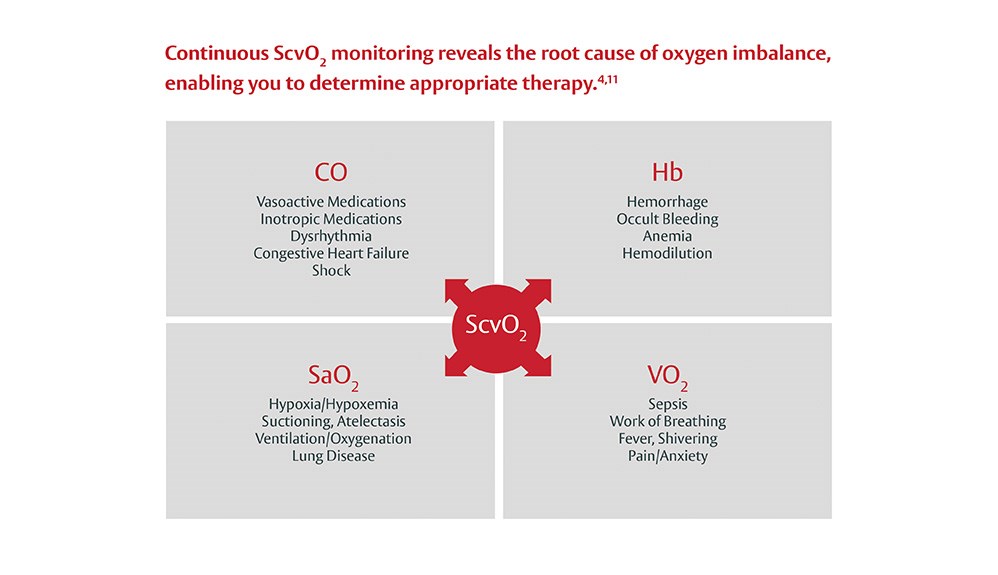
持续ScvO2监测可以揭示氧失衡的根源,让您能够积极地确定合适的疗法。4、11实时了解心排量是否充足可以让您即时评估患者的临床治疗反应性,−让您在组织缺氧和各阶段的脓毒症防治上始终保持主动。12
持续ScvO2监测可以指导治疗,让早期干预成为可能4、5
您可以按照ACCM-PALS临床实践参数来优化儿科和新生儿脓毒性休克患者的血液动力学管理13
清楚洞悉。保持主动。
PediaSat 血氧饱和度导管为氧供不足或受损提供明确的早期预警4-6、8、10
ScvO2的连续测量,加上器官灌注的其他度量(生命体征、乳酸等)可以可靠地监测心循环功能。17
- 发现全身氧供、氧摄取的急剧变化14
- 发现间歇式采样发现不了的全身氧供的下降9
- 评价常规干预的影响(如抽吸、沐浴、翻身)18
可优化复杂儿科患者的血液动力学管理。
- 先天性心脏病和其他复杂的心脏病患者19
- 脓毒症和脓毒性休克20
- 急性呼吸窘迫综合征(ARDS)18
- 其他高危患者3、21
方便、准确、易操作。17、22、23
PediaSat血氧饱和度导管提供:
- 简便灵活−在标准的儿科穿刺部位,包括锁骨下和颈静脉,使用与其他中心穿刺线路相同的穿刺技术
- 连续的ScvO2监测、压力监测和液体复苏
- 准确的氧合状态4
- 用双管腔及三管腔进行监测及给液
联系销售代表
- Spenceley, N., et al. Continuous central venous saturations during pericardial tamponade case report. Pediatr Crit Care Med 2007, Vol. 8, No. 3,p18.2.153.
- Krahn, G., et al. Early clinical evaluation of the Edwards PediaSat™ oximetry catheter in pediatric patients. Pediatr Crit Care Med 2007, Vol. 8, No. 3,p18.2.152.
- Spenceley, N., et al. Continuous central venous saturation monitoring in pediatrics: a case report. Pediatr Crit Care Med 2008, Vol. 9, No. 2, p e13-e16.
- Reinhart K, et al. Continuous central venous and pulmonary artery oxygen saturation monitoring in the critically ill. Intensive Care Med. 2004;30(8):1572-8.
- Rivers EP, et al. Central venous oxygen saturation monitoring in the critically ill patient. Curr Opin Crit Care. 2001;7(3):204-11.
- Ingelmo P, et al. Importance of monitoring in high-risk surgical patients. Minerva Anestesiol. 2002;68(4):226-30.
- Pearse, R, et al. Changes in central venous saturation after major surgery, and association with outcome. Crit Care 2005;9(6):R694-91.
- Scalea, TM, et al. Central venous oxygen saturation: a useful clinical tool in trauma patients. J Trauma 1990;30(12):1539-43.
- Tweddell JS, et al. Patients at risk for low systemic oxygen delivery after the Norwood procedure. Ann Thorac Surg. 2000;69(6):1893-9.
- Ander, DS, et al. Undetected cardiogenic shock in patients with congestive heart failure presenting to the emergency department. Am J Cardiol 1998;82(7):888-91.
- Zaja J. Venous oximetry. Signa Vitae 2007;2(1):6-10.
- Tweddell, JS, et al. Mixed venous oxygen saturation monitoring after stage 1 palliation for hypoplastic left heart syndrome. Ann Thorac Surg 2007;84:1301-1311.
- Oliveira, CF, et al. An outcomes comparison of ACCM/PALS guidelines for pediatric septic shock with and without central venous oxygen saturation monitoring. Pediatr Crit Care Med 2007, Vol. 8,No. 3 (Suppl.).
- Tweddell JS, et al. Postoperative management in patients with complex congenital heart disease. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2002;5:187-205.
- Tweddell, JS, et al. Improved survival of patients undergoing palliation of hypoplastic left heart syndrome: lessons learned from 115 consecutive patients. Circulation 2002;106(12 Suppl 1):I82-9.
- Hoffman GM, et al. Venous saturation and the anaerobic threshold in neonates after the Norwood procedure for hypoplastic left heart syndrome. Ann Thorac Surg. 2000;70(5): 1515-21.
- Mahajan A, et al. An experimental and clinical evaluation of a novel central venous catheter with integrated oximetry for pediatric patients undergoing cardiac surgery. Pediatric Central Venous Oximetry. Anest Anal. 2007;Vol.105, No. 6, 1598.
- Sanders CL. Making clinical decisions using SvO2 in PICU patients. Dimens Crit Care Nurs. 1997;16(5):257-64.
- Chakravarti, S.B., et al. Multisite Near-Infrared Spectroscopy Predicts Elevated Blood Lactate Level in Children After Cardiac Surgery. Journal of Cardiothoracic and Vascular Anesthesia. 2009.
- Lemson et al. Advanced hemodynamic monitoring in critically ill patients. Pediatrics. 2011.
- Ranucci et al. Central venous oxygen saturation and blood lactate levels during cardiopulmonary bypass are associated with outcome after pediatric cardiac surgery. Critical Care 2010.
- Vallet B, et al. Venous oxygen saturation as a physiologic transfusion trigger. Crit Care. 2010;14:213.
- Clinical PreSep PediaSat Clinical Evaluation Report.
Please update your browser

Please update to a current version of your preferred browser, this site will perform effectively on the following:




If you are on a computer, that is maintained by an admin and you cannot install a new browser, ask your admin about it. If you can't change your browser because of compatibility issues, think about installing a second browser for browsing and keep this old one for compatibility